Dr. Sanjay Agrawal
Leading Pharmaceutical consultant and editor-in chief of IJMToday
Hypertension is a chronic medical condition characterised by higher pressure exerted by blood against the walls of the arteries. According to the American Heart Association guidelines hypertension is mainly classified into two stages. Stage 1 and stage 2 is characterised by systolic blood pressure 130-139mmHg and ≥140mmHg, diastolic pressure 80-89mmHg and ≥90mmHg respectively(https://www.cdc.gov/bloodpressure/facts.htm). Physiological mechanisms which govern the development of hypertension include cardiac output and peripheral vascular resistance, renin-angiotensin-aldosterone system, autonomic nervous system, endothelial dysfunction and the release of vasodilators like nitric oxide, bradykinin, hypercoagulability, insulin sensitivity, intrauterine factors, diastolic dysfunction and genetic factors(Beevers et al., 2001).
Through their positive effects on blood pressure, a high consumption of omega-3 PUFAs has been linked to cardiovascular protective benefits, enhancing endothelial function, and lowering atherosclerosis. In addition, they also have effect on their lipid profile, platelet aggregation, and characteristics that reduce inflammation. α-linolenic acid (ALA) undergoes desaturation in the presence of 6-desaturase, 5-desaturase and elongation in the presence of elongase to form eicosapentaenoic acid (EPA), a precursor of 3 series of prostaglandins, 5 series of leukotrienes and thromboxanes. These 3 series PGs are less potent when compared to series 2 obtained through arachidonic acid and hence they have antagonistic effects on vascular tone, platelet aggregation, and inflammation. EPA further undergoes desaturation and elongation in the presence of 4-desaturase and elongase respectively resulting in the formation of docosahexaenoic acid (DHA). EPA and DHA are precursors for lipoxins, resolvins and protectins which are involved in mediating inflammation, vascular tone and blood pressure as given in Figure 1. But these desaturation and elongation reactions are slow in human body which attribute to its lesser efficacy and in addition to this, metabolic pathway of omega-6 FA interfere with EPA and DHA formation, thereby affecting peripheral vascular resistance and blood pressure. Also, omega-3 FA suppress the aldosterone secretion and enhance nitric oxide production controlling hypertension. Various studies have proved the cardioprotective action of omega-3 FA in lowering systemic vascular resistance, reducing heart rate and improving cardiac diastole thereby lowering risk of cardiac death and possibly ischaemic stroke, heart failure, and non-fatal coronary events (Cabo et al., 2012).
Mori et al have reported a significant effect of EPA and DHA in lowering blood pressure via improving endothelial and smooth muscle functions. Incorporation of DHA into the endothelial membranes increased membrane fluidity, calcium influx, synthesis and release of NO, enhanced release of vasodilatory prostanoids and endothelial derived hyperpolarising factor. They also reported the a reduction in leptin levels thereby causing weight loss in 112/hypertensive patients, reducing ambulatory blood pressure and heart rate (Mori, 2006). Hence it can be concluded that omega-3 fatty acids play a vital role in the treatment of hypertension and in turn cardio protection.
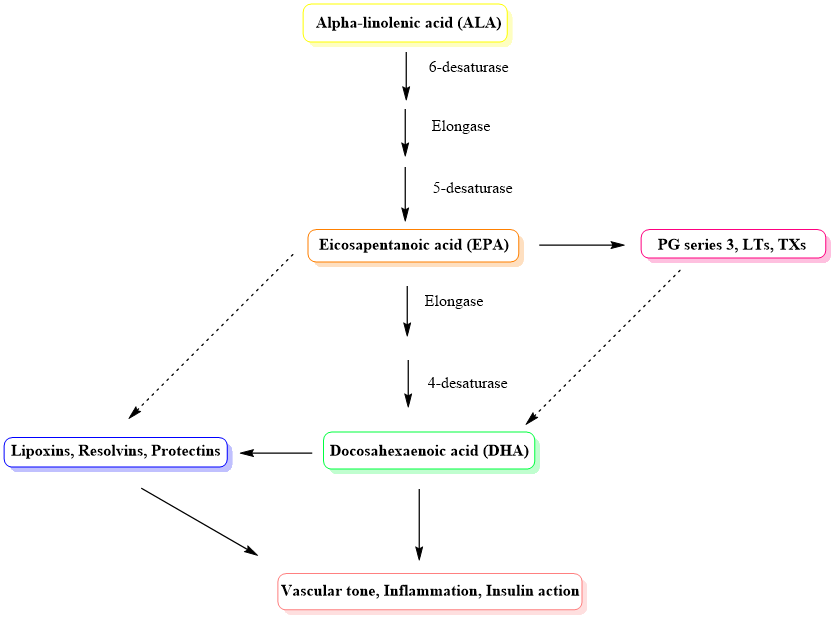
Figure1. Metabolic pathway of omega-3 FA